Health psychology is a subfield of psychology that examines how biological, psychological, and social factors influence health, illness, and health-related behaviors. Rather than viewing health as simply the absence of disease, health psychologists take a holistic approach — studying how our thoughts, emotions, behaviors, and social environments interact to affect our physical well-being.
The Biopsychosocial Model
The biopsychosocial model (George Engel, 1977) is the foundational framework of health psychology. It proposes that health and illness result from the interaction of three factors:
Biological factors: Genetics, brain chemistry, immune system functioning, hormones, pathogens, and physiological processes.
Psychological factors: Thoughts, emotions, coping styles, personality traits, stress levels, self-efficacy, and health beliefs.
Social factors: Socioeconomic status, cultural norms, family relationships, social support networks, access to healthcare, and peer influences.
This model replaced the older biomedical model, which explained disease purely in biological terms and ignored psychological and social contributors.
The Biopsychosocial Model: Health results from the interaction of biological, psychological, and social factors. (Wikimedia Commons, CC BY-SA 4.0)
Stress and Health
Stress is the body's response to perceived threats or challenges. While short-term stress can be adaptive (helping us respond to danger), chronic stress weakens the immune system, increases vulnerability to illness, and contributes to cardiovascular disease, depression, and other conditions.
Types of Stress
Eustress: Positive, motivating stress that enhances performance (e.g., excitement before a competition).
Distress: Negative stress that causes anxiety, impairs performance, and harms health.
Acute Stress: Short-term stress in response to an immediate threat or challenge.
Death of a loved one, divorce, job loss, moving. Measured by the Holmes & Rahe Social Readjustment Rating Scale (SRRS).
Daily Hassles
Traffic, deadlines, arguments, financial worries. Research shows daily hassles can be more predictive of health problems than major life events (Lazarus).
Stress and the Immune System — Psychoneuroimmunology
Psychoneuroimmunology (PNI) studies the interaction between psychological processes, the nervous system, and the immune system. Key findings include:
Chronic stress suppresses lymphocyte (white blood cell) activity, making the body more susceptible to infections and disease.
The HPA axis (hypothalamic-pituitary-adrenal axis) releases cortisol during stress. Prolonged cortisol elevation damages the hippocampus, suppresses immune function, and increases abdominal fat storage.
Stress can worsen conditions like heart disease, diabetes, and autoimmune disorders.
Coping with Stress
Coping Strategy
Description
Example
Problem-Focused Coping
Directly addressing the stressor by taking action to reduce or eliminate it. Most effective when the situation is controllable.
Creating a study schedule to manage exam stress.
Emotion-Focused Coping
Managing the emotional response to stress rather than the stressor itself. More common when the situation is uncontrollable.
Practicing meditation after the death of a loved one.
Social Support
Seeking comfort, advice, or practical help from others. One of the strongest predictors of positive health outcomes.
Talking to friends about a stressful work situation.
Exercise
Regular physical activity reduces cortisol, increases endorphins, and improves mood, sleep, and immune function.
Going for a run to relieve tension after a difficult day.
Perceived Control: People who believe they have control over their health (internal health locus of control) are more likely to engage in health-promoting behaviors.
Key Takeaway: Health psychology uses the biopsychosocial model to explain how biological, psychological, and social factors interact to influence health. Chronic stress — through the HPA axis and cortisol — weakens the immune system. Coping strategies (problem-focused vs. emotion-focused) and personality types (Type A hostility) are high-frequency AP exam topics.
🌞 5.2 Positive Psychology
Positive psychology is a relatively new branch of psychology founded by Martin Seligman in the late 1990s. Rather than focusing exclusively on mental illness and dysfunction, positive psychology studies the conditions and processes that contribute to human flourishing — optimal well-being, happiness, and the fulfillment of human potential.
Seligman’s PERMA Model
Seligman proposed the PERMA model as a framework for well-being, identifying five core elements that contribute to a flourishing life:
Element
Description
Positive Emotions
Experiencing joy, gratitude, hope, love, and other positive feelings. Goes beyond momentary pleasure to sustained positive affect.
Engagement
Being fully absorbed in activities — achieving a state of flow (Csikszentmihalyi). Occurs when challenge and skill level are well-matched.
Relationships
Positive, meaningful connections with others. Social bonds are among the strongest predictors of well-being and longevity.
Meaning
Having a sense of purpose — belonging to and serving something greater than the self (e.g., religion, community, a cause).
Accomplishment
Pursuing achievement and mastery for its own sake. A sense of competence and progress toward meaningful goals.
Seligman’s PERMA Model: Five pillars of well-being — Positive Emotions, Engagement, Relationships, Meaning, and Accomplishment. (Wikimedia Commons, CC BY-SA 4.0)
Flow (Mihaly Csikszentmihalyi)
Flow is a mental state of complete immersion and focused energy in an activity. Csikszentmihalyi described it as being “in the zone.” Flow occurs when:
The challenge of the task matches your skill level — not too easy (boredom) and not too hard (anxiety).
You have clear goals and receive immediate feedback.
You lose track of time and self-consciousness.
Flow is associated with increased happiness, creativity, and intrinsic motivation. It can occur in work, sports, art, music, or any deeply engaging activity.
Subjective Well-Being (SWB)
Subjective well-being refers to how people evaluate their own lives — their overall life satisfaction and the balance of positive to negative emotions. Research findings include:
Adaptation-Level Phenomenon: People tend to adapt to both positive and negative events, returning to a baseline level of happiness over time. Lottery winners and accident victims both return close to their original happiness levels (Brickman, Coates, & Janoff-Bulman, 1978).
Relative Deprivation: Happiness is influenced by comparing ourselves to others. Feeling worse off than those around us decreases well-being, even if our absolute situation is good.
Set-Point Theory of Happiness: Each person has a genetically influenced baseline level of happiness to which they tend to return after positive or negative experiences.
Character Strengths and Virtues
Seligman and Christopher Peterson developed the VIA (Values in Action) Classification of Strengths — a positive psychology counterpart to the DSM. It identifies 24 character strengths organized under 6 core virtues:
Wisdom (creativity, curiosity, open-mindedness, love of learning, perspective)
Transcendence (appreciation of beauty, gratitude, hope, humor, spirituality)
Resilience and Growth Mindset
Resilience: The ability to recover from adversity, trauma, or significant stress. Protective factors include strong social support, optimism, and effective coping strategies.
Post-Traumatic Growth: Some individuals not only recover from trauma but experience positive psychological changes — greater appreciation for life, improved relationships, increased personal strength, and new possibilities.
Growth Mindset (Carol Dweck): The belief that abilities and intelligence can be developed through effort and learning. Contrasts with a fixed mindset (believing abilities are innate and unchangeable). Growth mindset promotes resilience, motivation, and academic achievement.
Gratitude, Mindfulness, and Well-Being Interventions
Gratitude exercises: Keeping a gratitude journal or writing gratitude letters has been shown to increase well-being and decrease depressive symptoms.
Mindfulness meditation: Paying attention to the present moment without judgment. Reduces stress, anxiety, and depression while increasing emotional regulation and life satisfaction.
Acts of kindness: Performing intentional acts of kindness for others increases the giver's well-being.
Key Takeaway: Positive psychology studies what makes life worth living. The PERMA model, flow, subjective well-being (including the adaptation-level phenomenon), and growth mindset are key concepts. This is a new addition to the AP Psychology framework — expect exam questions on Seligman, Csikszentmihalyi, and Dweck.
🔍 5.3 Explaining and Classifying Psychological Disorders
A psychological disorder (mental disorder) is a syndrome characterized by a clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning. Understanding how disorders are defined, explained, and classified is essential for both diagnosis and treatment.
Defining “Abnormal” Behavior
Psychologists use several criteria to determine whether behavior is abnormal. No single criterion is sufficient on its own — clinicians consider multiple factors:
Criterion
Description
Limitation
Statistical Rarity
Behavior that deviates significantly from the statistical average.
Disorders result from failure to meet one’s potential or conditions of worth that distort self-concept.
Incongruence between real self and ideal self; lack of unconditional positive regard. Treatment: client-centered therapy.
Sociocultural
Disorders are influenced by social and cultural context — poverty, discrimination, cultural norms.
Social determinants of health; culture-bound syndromes; labeling effects. Treatment: family/community interventions.
Biopsychosocial
Disorders result from the interaction of biological, psychological, and social factors.
Integrates all perspectives. The dominant modern approach.
The Diathesis-Stress Model
The diathesis-stress model proposes that psychological disorders develop when a person has a biological or psychological vulnerability (diathesis) that is triggered by environmental stressors. Neither the vulnerability alone nor the stress alone is sufficient — both are needed. This helps explain why some people develop disorders while others with the same genetic predisposition do not.
The DSM-5-TR: Classification of Disorders
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR), published by the American Psychiatric Association (2022), is the standard classification system used in the United States for diagnosing psychological disorders.
Contains descriptions, symptoms, and diagnostic criteria for over 300 disorders.
Uses a categorical approach — a person either meets criteria for a disorder or does not — though many researchers argue for a dimensional approach (viewing symptoms on a continuum).
Criticisms: Potential for over-diagnosis, cultural bias, labeling effects (Rosenhan’s “Being Sane in Insane Places” study, 1973), reliability concerns, and the influence of pharmaceutical companies.
Labeling and Stigma
Rosenhan’s Study (1973): Pseudopatients who reported hearing voices were admitted to psychiatric hospitals and diagnosed with schizophrenia. Once labeled, their normal behaviors were interpreted through the lens of their diagnosis. This demonstrated the power of labeling and the difficulty of distinguishing “sane” from “insane” in institutional settings.
Stigma: People with mental illness often face discrimination, social rejection, and reduced opportunities. Stigma can prevent people from seeking treatment.
Self-fulfilling prophecy: Being labeled with a disorder can shape how others treat the person, potentially reinforcing the very behaviors associated with the diagnosis.
Key Takeaway: The biopsychosocial model and diathesis-stress model are the dominant frameworks for understanding psychological disorders. The DSM-5-TR provides diagnostic criteria but has limitations (labeling effects, cultural bias). Know all seven theoretical perspectives and Rosenhan’s study for the AP exam.
📈 5.4 Selection of Categories of Psychological Disorders
The AP Psychology exam requires knowledge of major categories of psychological disorders as classified by the DSM-5-TR. Below is a comprehensive overview of the most commonly tested disorder categories, their symptoms, causes, and key research.
Neurodevelopmental Disorders
Disorder
Key Features
Additional Information
Attention-Deficit/Hyperactivity Disorder (ADHD)
Persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning. Three presentations: predominantly inattentive, predominantly hyperactive-impulsive, or combined.
Onset before age 12. More commonly diagnosed in males. Associated with differences in prefrontal cortex and dopamine functioning. Treated with stimulant medications (e.g., methylphenidate) and behavioral therapy.
Autism Spectrum Disorder (ASD)
Persistent deficits in social communication and interaction across multiple contexts, along with restricted, repetitive patterns of behavior, interests, or activities.
Exists on a spectrum from mild to severe. Symptoms present in early development. Not caused by vaccines (this myth has been thoroughly debunked). Associated with genetic factors and differences in brain connectivity.
Schizophrenia Spectrum Disorders
Schizophrenia is a severe disorder characterized by disturbances in thought, perception, emotion, and behavior. Symptoms are categorized as:
Symptom Type
Description
Examples
Positive Symptoms
Excesses or distortions of normal functioning (things that are “added”).
Reductions in normal functioning (things that are “taken away”).
Flat affect (reduced emotional expression); alogia (poverty of speech); avolition (lack of motivation); social withdrawal; anhedonia (inability to experience pleasure).
Genetics: Strong genetic component — concordance rate is ~48% for identical twins vs. ~17% for fraternal twins. Having a biological relative with schizophrenia significantly increases risk.
Brain Abnormalities: Enlarged ventricles, reduced cortical gray matter, and abnormalities in the prefrontal cortex and temporal lobes.
Prenatal Factors: Viral infections during pregnancy, birth complications, and malnutrition increase risk.
Bipolar and Depressive Disorders
Major Depressive Disorder (MDD)
Characterized by persistent depressed mood or loss of interest/pleasure (anhedonia) lasting at least two weeks, along with at least five of the following symptoms:
Significant weight change or appetite change
Insomnia or hypersomnia
Psychomotor agitation or retardation
Fatigue or loss of energy
Feelings of worthlessness or excessive guilt
Difficulty concentrating or making decisions
Recurrent thoughts of death or suicidal ideation
Causes: Low levels of serotonin and norepinephrine; genetic predisposition; Beck’s cognitive triad (negative views of self, world, and future); learned helplessness (Seligman); stressful life events.
Bipolar Disorder
Characterized by alternating episodes of mania (or hypomania) and depression.
Manic episodes: Abnormally elevated or irritable mood, grandiosity, decreased need for sleep, pressured speech, racing thoughts, risk-taking behavior, increased goal-directed activity.
Bipolar I: Full manic episodes (may or may not include depressive episodes).
Bipolar II: Hypomanic episodes (less severe mania) plus major depressive episodes.
Beck’s Cognitive Triad: Depression involves negative views of the self, the world, and the future. (Wikimedia Commons, CC BY-SA 4.0)
Anxiety Disorders
Anxiety disorders involve excessive fear or anxiety that is disproportionate to the actual threat and interferes with daily functioning.
Disorder
Key Features
Generalized Anxiety Disorder (GAD)
Persistent, excessive worry about multiple areas of life (health, finances, work) for at least 6 months. Accompanied by restlessness, fatigue, difficulty concentrating, muscle tension, and sleep disturbance.
Specific Phobia
Intense, irrational fear of a specific object or situation (e.g., spiders, heights, flying). Leads to avoidance behavior. Learned through classical conditioning or observational learning.
Social Anxiety Disorder
Intense fear of social situations where one might be scrutinized, judged, or embarrassed. Leads to avoidance of social interactions.
Panic Disorder
Recurrent, unexpected panic attacks — sudden surges of intense fear with physical symptoms (racing heart, shortness of breath, dizziness, chest pain). Fear of future attacks.
Agoraphobia
Fear or avoidance of situations where escape might be difficult (e.g., crowds, public transportation, open spaces). Often develops after panic attacks.
Obsessive-Compulsive and Related Disorders
Obsessive-Compulsive Disorder (OCD): Characterized by obsessions (unwanted, intrusive, recurring thoughts that cause anxiety) and compulsions (repetitive behaviors performed to reduce the anxiety caused by obsessions). Example: Fear of contamination (obsession) → excessive handwashing (compulsion).
Body Dysmorphic Disorder: Preoccupation with perceived flaws in physical appearance that are not observable or appear slight to others.
Trauma- and Stressor-Related Disorders
Post-Traumatic Stress Disorder (PTSD): Develops after exposure to a traumatic event (combat, assault, disaster). Symptoms include intrusive memories (flashbacks, nightmares), avoidance of trauma-related stimuli, negative changes in cognition and mood, and hyperarousal (exaggerated startle response, hypervigilance, sleep disturbance). Symptoms persist for more than one month.
Dissociative Disorders
Dissociative Identity Disorder (DID): Formerly “multiple personality disorder.” Characterized by the presence of two or more distinct personality states. Often linked to severe childhood trauma. Controversial — some argue it is iatrogenic (therapist-created).
Dissociative Amnesia: Inability to recall important personal information, usually related to a traumatic event. May include dissociative fugue (sudden, unexpected travel away from home with amnesia for one’s past).
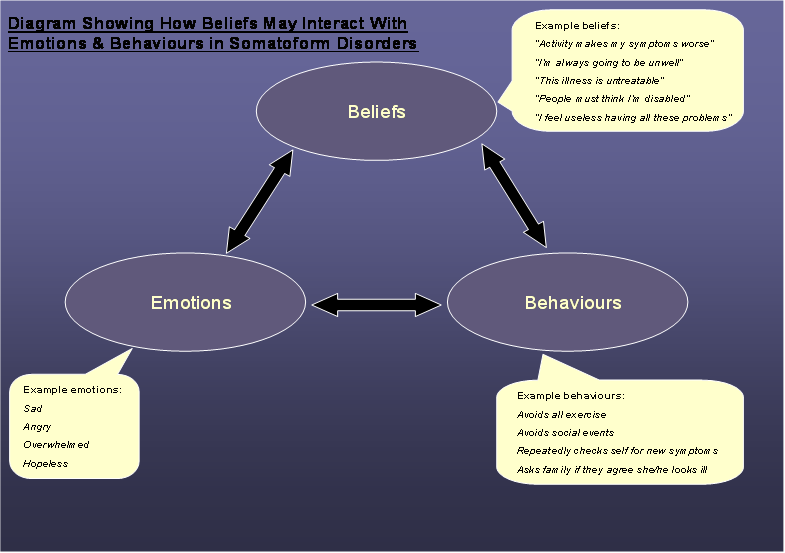
Somatic Symptom and Related Disorders
Somatic Symptom Disorder: One or more physical symptoms (pain, fatigue) accompanied by excessive thoughts, feelings, or behaviors related to those symptoms. The distress is genuine, even if no medical explanation is found.
Illness Anxiety Disorder: Formerly “hypochondriasis.” Preoccupation with having or developing a serious illness despite minimal or no symptoms.
Conversion Disorder: Neurological symptoms (blindness, paralysis, numbness) without a medical cause, often following psychological stress.
Feeding and Eating Disorders
Disorder
Key Features
Anorexia Nervosa
Restriction of energy intake leading to significantly low body weight; intense fear of gaining weight; distorted body image. Highest mortality rate of any mental disorder.
Bulimia Nervosa
Recurrent episodes of binge eating followed by compensatory behaviors (purging, excessive exercise, fasting). Individuals are often at or near normal weight.
Binge-Eating Disorder
Recurrent episodes of binge eating without compensatory behaviors. Associated with distress, shame, and obesity.
Personality Disorders
Personality disorders are enduring, inflexible patterns of inner experience and behavior that deviate markedly from cultural expectations. The DSM-5-TR organizes them into three clusters:
Antisocial PD (disregard for others’ rights, lack of remorse, deceitfulness); Borderline PD (instability in relationships, self-image, and emotions; fear of abandonment); Histrionic PD; Narcissistic PD.
Cluster C (Anxious/Fearful)
Behavior is characterized by anxiety and fearfulness.
Substance Use Disorder: A pattern of substance use leading to clinically significant impairment or distress. Key criteria include tolerance (needing more of the substance for the same effect), withdrawal (physical/psychological symptoms when stopping), failed attempts to cut down, and continued use despite negative consequences.
Social factors: Peer pressure, socioeconomic stress, family history, cultural attitudes toward substance use.
Key Takeaway: The AP exam tests multiple disorder categories in depth. For each disorder, know the key symptoms, biological and psychological causes, and any landmark research. Schizophrenia (positive vs. negative symptoms, dopamine hypothesis), major depression (serotonin, Beck’s cognitive triad), and anxiety disorders are among the most heavily tested.
💊 5.5 Treatment of Psychological Disorders
Treatment approaches for psychological disorders fall into two broad categories: psychotherapy (talk therapy) and biomedical therapy (medications and medical procedures). Many clinicians use an eclectic approach, combining techniques from multiple therapeutic orientations based on the client’s needs.
Psychotherapy Approaches
Approach
Key Theorist(s)
Core Techniques
Goal
Psychoanalytic / Psychodynamic
Sigmund Freud
Free association (saying whatever comes to mind); dream analysis; transference (projecting feelings onto the therapist); interpretation of resistance.
Bring unconscious conflicts into conscious awareness to resolve them.
Humanistic / Client-Centered
Carl Rogers
Active listening; unconditional positive regard; empathy; genuineness (congruence). Non-directive — the therapist does not interpret or advise.
Promote self-awareness, personal growth, and self-acceptance in a safe, supportive environment.
Change both distorted thoughts and maladaptive behaviors. The most empirically supported therapy for many disorders (depression, anxiety, PTSD, OCD).
Group, Family, and Community Approaches
Group Therapy: A therapist works with multiple clients simultaneously. Benefits include social support, shared experiences, diverse perspectives, and cost-effectiveness. Self-help groups (e.g., Alcoholics Anonymous) provide peer support without a professional therapist.
Family Therapy: Treats the family as a system. Focuses on improving communication patterns, resolving conflicts, and addressing dysfunctional family dynamics that contribute to individual members’ problems.
Community Mental Health: The deinstitutionalization movement (1960s–70s) shifted care from psychiatric hospitals to community-based treatment. Community mental health centers provide outpatient therapy, crisis intervention, and preventive services. However, deinstitutionalization also contributed to homelessness among those with severe mental illness who lacked adequate community support.
Evaluating Psychotherapy Effectiveness
Meta-analyses consistently show that psychotherapy is more effective than no treatment for most disorders.
Common factors: Regardless of the specific approach, successful therapy shares common elements — a strong therapeutic alliance (trusting relationship between therapist and client), hope and expectation of improvement, and a structured rationale for the treatment.
Evidence-based practice: Integrating the best available research evidence with clinical expertise and patient preferences. CBT has the strongest evidence base for many disorders.
CBT Framework: Thoughts, feelings, and behaviors influence each other. Cognitive-behavioral therapy targets all three. (Wikimedia Commons, CC BY-SA 3.0)
Increase dopamine and norepinephrine activity in the prefrontal cortex.
ADHD. Paradoxically, stimulants improve focus and reduce hyperactivity.
Brain Stimulation Therapies
Therapy
Description
Used For
Electroconvulsive Therapy (ECT)
Brief electrical stimulation of the brain while the patient is under anesthesia. Induces a controlled seizure. Administered 2–3 times per week for several weeks.
Severe, treatment-resistant depression; acute suicidal ideation. One of the most effective treatments for severe depression. Side effect: temporary memory loss.
Transcranial Magnetic Stimulation (TMS)
Uses magnetic pulses to stimulate nerve cells in the brain, particularly the prefrontal cortex. Non-invasive; no anesthesia required.
Treatment-resistant depression. Fewer side effects than ECT.
Experimental treatment for severe OCD, treatment-resistant depression.
Psychosurgery
Lobotomy: A historical procedure (developed by Egas Moniz in the 1930s; popularized by Walter Freeman) that severed connections to the prefrontal cortex. Caused severe side effects (personality changes, cognitive impairment, death). Now considered unethical and no longer performed.
Modern psychosurgery is extremely rare, highly precise, and used only as a last resort for severe, treatment-resistant cases.
Therapeutic Approaches Matched to Disorders
Disorder
Most Effective Treatment(s)
Major Depression
CBT + SSRIs (combination is most effective); ECT for severe/treatment-resistant cases.
Bipolar Disorder
Mood stabilizers (lithium) + psychotherapy.
Schizophrenia
Antipsychotic medication + psychosocial rehabilitation and skills training.
Anxiety Disorders
CBT (especially exposure therapy) + SSRIs or anxiolytics for severe cases.
OCD
CBT with exposure and response prevention (ERP) + SSRIs.
PTSD
Trauma-focused CBT; EMDR (Eye Movement Desensitization and Reprocessing); SSRIs.
Specific Phobias
Systematic desensitization; exposure therapy. Medication is generally not first-line.
ADHD
Stimulant medication + behavioral interventions.
Key Takeaway: Know the major therapy approaches (psychodynamic, humanistic, behavioral, cognitive, CBT) and their key techniques. For biomedical treatments, know the drug classes (SSRIs, antipsychotics, mood stabilizers, anxiolytics) and their mechanisms. CBT is the most empirically supported therapy. ECT is effective for severe depression. The AP exam frequently asks you to match therapies to disorders.
📚 Key Vocabulary — Unit 5
Term
Definition
Health Psychology
Subfield studying how biological, psychological, and social factors influence health, illness, and health-related behaviors.
Biopsychosocial Model
Framework proposing that health and illness result from the interaction of biological, psychological, and social factors (Engel, 1977).
Psychoneuroimmunology
Study of how psychological processes, the nervous system, and the immune system interact to affect health.
Cortisol
Stress hormone released by the adrenal glands via the HPA axis; chronic elevation suppresses immune function.
Coping strategy that directly addresses the stressor by taking action to reduce or eliminate it.
Emotion-Focused Coping
Coping strategy that manages the emotional response to stress rather than the stressor itself.
Type A Personality
Personality pattern characterized by competitiveness, hostility, impatience, and time urgency; linked to coronary heart disease.
Hardy Personality
Personality style characterized by commitment, control, and challenge; associated with resilience under stress (Kobasa).
Positive Psychology
Branch of psychology studying conditions and processes that contribute to human flourishing and optimal well-being (Seligman).
PERMA Model
Seligman’s framework for well-being: Positive Emotions, Engagement, Relationships, Meaning, and Accomplishment.
Flow
State of complete immersion and focused energy in an activity when challenge matches skill level (Csikszentmihalyi).
Subjective Well-Being
A person’s evaluation of their own life — life satisfaction and the balance of positive to negative emotions.
Adaptation-Level Phenomenon
Tendency to adapt to new circumstances, returning to a baseline level of happiness after positive or negative events.
Growth Mindset
Belief that abilities and intelligence can be developed through effort and learning (Dweck).
Resilience
The ability to recover from adversity, trauma, or significant sources of stress.
DSM-5-TR
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision — the standard classification system for psychological disorders in the U.S.
Diathesis-Stress Model
Model proposing that disorders develop when a biological/psychological vulnerability is triggered by environmental stress.
Schizophrenia
Severe disorder characterized by positive symptoms (hallucinations, delusions) and negative symptoms (flat affect, avolition).
Hallucination
A false sensory experience (e.g., hearing voices) that occurs without an external stimulus.
Delusion
A false belief held despite contradictory evidence (e.g., paranoid delusions, grandiose delusions).
Dopamine Hypothesis
Theory that schizophrenia is associated with excessive dopamine activity; basis for antipsychotic medications.
Major Depressive Disorder
Mood disorder involving persistent depressed mood or loss of interest/pleasure for at least two weeks with additional symptoms.
Bipolar Disorder
Mood disorder characterized by alternating episodes of mania (elevated mood, energy) and depression.
Generalized Anxiety Disorder
Excessive, persistent worry about multiple areas of life for at least six months.
Panic Disorder
Recurrent, unexpected panic attacks — sudden surges of intense fear with physical symptoms.
Obsessive-Compulsive Disorder
Disorder characterized by obsessions (unwanted, intrusive thoughts) and compulsions (repetitive behaviors to reduce anxiety).
PTSD
Post-Traumatic Stress Disorder — develops after trauma; symptoms include flashbacks, avoidance, negative mood changes, and hyperarousal.
Dissociative Identity Disorder
Presence of two or more distinct personality states; often linked to severe childhood trauma.
Anorexia Nervosa
Eating disorder involving restriction of food intake, significantly low body weight, and distorted body image.
Bulimia Nervosa
Eating disorder involving binge eating followed by compensatory behaviors (purging, excessive exercise).
Antisocial Personality Disorder
Personality disorder characterized by disregard for others’ rights, lack of remorse, deceitfulness, and impulsivity.
Cognitive-Behavioral Therapy (CBT)
Therapy combining cognitive restructuring (changing distorted thoughts) with behavioral techniques; the most empirically supported approach.
Systematic Desensitization
Behavioral technique pairing progressive relaxation with gradual exposure to feared stimuli to reduce phobic anxiety (Wolpe).
SSRI
Selective Serotonin Reuptake Inhibitor — antidepressant that blocks reuptake of serotonin (e.g., Prozac, Zoloft).
Antipsychotic
Medication that blocks dopamine receptors; used to treat schizophrenia and psychotic symptoms.
Electroconvulsive Therapy (ECT)
Brain stimulation therapy using brief electrical current under anesthesia; effective for severe, treatment-resistant depression.
Therapeutic Alliance
The trusting, collaborative relationship between therapist and client — a strong predictor of positive therapy outcomes.
Deinstitutionalization
Movement to shift care of people with severe mental illness from psychiatric hospitals to community-based treatment.
Eclectic Approach
Therapeutic approach that draws from multiple therapy orientations based on the client’s individual needs.
Tardive Dyskinesia
Involuntary repetitive movements (often of the face/tongue) caused by long-term use of first-generation antipsychotics.
✍️ Practice Multiple-Choice Questions (25)
Click Show Answer to reveal the correct response and explanation.
1. The biopsychosocial model proposes that health and illness are best understood by examining:
A) Only biological and genetic factors
B) The interaction of biological, psychological, and social factors
C) Only psychological factors such as personality and coping
D) Environmental factors and public health policies
Answer: B) The biopsychosocial model (Engel, 1977) integrates biological, psychological, and social factors to provide a holistic understanding of health and illness, replacing the older biomedical model that focused only on biology.
2. Which of the following is the BEST example of problem-focused coping?
A) Meditating to reduce anxiety before a job interview
B) Talking to a friend about your feelings after a breakup
C) Creating a detailed study plan to prepare for a difficult exam
D) Going for a run to relieve stress after a bad day at work
Answer: C) Problem-focused coping involves directly addressing the stressor itself. Creating a study plan is an active attempt to manage the source of stress (the difficult exam). The other options are examples of emotion-focused coping.
3. Research in psychoneuroimmunology has demonstrated that chronic stress:
A) Strengthens the immune system by increasing cortisol production
B) Has no measurable effect on immune functioning
C) Suppresses lymphocyte activity and increases vulnerability to illness
D) Only affects mental health, not physical health
Answer: C) Chronic stress suppresses the immune system by reducing lymphocyte (white blood cell) activity, making the body more susceptible to infections and disease. Prolonged cortisol elevation is the primary mechanism.
4. According to Friedman and Rosenman, which component of the Type A personality is most strongly linked to coronary heart disease?
A) Time urgency
B) Competitiveness
C) Hostility
D) Ambitiousness
Answer: C) Research has identified hostility as the “toxic” component of the Type A personality pattern most strongly associated with increased risk of coronary heart disease.
5. Martin Seligman’s PERMA model includes all of the following elements EXCEPT:
A) Positive Emotions
B) Resilience
C) Meaning
D) Accomplishment
Answer: B) PERMA stands for Positive Emotions, Engagement, Relationships, Meaning, and Accomplishment. Resilience is an important concept in positive psychology but is not one of the five PERMA elements.
6. Csikszentmihalyi’s concept of “flow” is most likely to occur when:
A) The task is extremely easy and requires minimal effort
B) The challenge of the task matches the person’s skill level
C) The person is externally motivated by rewards
D) The person is multitasking on several activities simultaneously
Answer: B) Flow occurs when the challenge level matches the person’s skill level — the task is neither too easy (leading to boredom) nor too difficult (leading to anxiety). It requires focused attention on a single activity.
7. The adaptation-level phenomenon suggests that lottery winners will:
A) Remain permanently happier than they were before winning
B) Become progressively less happy over the years
C) Eventually return to approximately their pre-winning level of happiness
D) Experience severe depression after the initial excitement fades
Answer: C) The adaptation-level phenomenon predicts that people adapt to changed circumstances and return to their baseline level of happiness. Research shows that lottery winners’ happiness levels return close to their pre-winning levels over time.
8. The diathesis-stress model proposes that psychological disorders develop when:
A) A person experiences extreme stress regardless of their genetic makeup
B) A biological or psychological vulnerability is triggered by environmental stressors
C) A person’s genes directly cause the disorder without environmental influence
D) Social and cultural factors alone determine who develops a disorder
Answer: B) The diathesis-stress model proposes that a combination of biological/psychological vulnerability (diathesis) and environmental stressors is needed for a disorder to develop. Neither factor alone is sufficient.
9. Rosenhan’s “Being Sane in Insane Places” study demonstrated that:
A) Psychiatric diagnosis is highly reliable and valid
B) Diagnostic labels can influence how behavior is perceived and interpreted
C) Patients in psychiatric hospitals receive excellent individualized care
D) The DSM provides clear boundaries between normal and abnormal behavior
Answer: B) Rosenhan’s pseudopatients were diagnosed with schizophrenia and their normal behaviors were then interpreted as symptoms of the disorder. This demonstrated the powerful influence of diagnostic labeling on perception.
10. Which of the following is a POSITIVE symptom of schizophrenia?
A) Flat affect
B) Avolition
C) Auditory hallucinations
D) Social withdrawal
Answer: C) Positive symptoms are excesses or distortions added to normal functioning. Auditory hallucinations (hearing voices) are the most common positive symptom. Flat affect, avolition, and social withdrawal are all negative symptoms (reductions in normal functioning).
11. The dopamine hypothesis of schizophrenia suggests that:
A) Schizophrenia is caused by too little dopamine activity
B) Excess dopamine activity contributes to the disorder, particularly positive symptoms
C) Dopamine has no role in schizophrenia
D) Low serotonin levels are the primary cause of schizophrenia
Answer: B) The dopamine hypothesis proposes that excessive dopamine activity, particularly in certain brain pathways, contributes to the positive symptoms of schizophrenia. This is supported by the effectiveness of antipsychotic drugs that block dopamine receptors.
12. According to Beck’s cognitive theory, depression is maintained by negative views of:
A) The self, others, and authority figures
B) The self, the world, and the future
C) Childhood, relationships, and career success
D) Genetics, neurotransmitters, and brain structure
Answer: B) Beck’s cognitive triad identifies three types of negative thinking that characterize depression: negative views of the self (“I’m worthless”), the world (“Everything is terrible”), and the future (“Things will never get better”).
13. A person who experiences recurrent panic attacks followed by persistent worry about having another attack would most likely be diagnosed with:
A) Generalized anxiety disorder
B) Social anxiety disorder
C) Panic disorder
D) Specific phobia
Answer: C) Panic disorder is characterized by recurrent, unexpected panic attacks AND persistent concern or worry about additional attacks. GAD involves chronic worry about multiple topics, not specifically about panic attacks.
14. Which eating disorder has the HIGHEST mortality rate of any psychological disorder?
A) Binge-eating disorder
B) Bulimia nervosa
C) Anorexia nervosa
D) Avoidant/restrictive food intake disorder
Answer: C) Anorexia nervosa has the highest mortality rate of any psychological disorder, due to the medical complications of severe malnutrition and the risk of suicide.
15. Obsessive-compulsive disorder (OCD) is characterized by:
A) Alternating episodes of mania and depression
B) Unwanted, intrusive thoughts and repetitive behaviors performed to reduce anxiety
C) Persistent worry about multiple areas of life
D) Hallucinations and delusions
Answer: B) OCD involves obsessions (unwanted, intrusive, recurring thoughts that cause anxiety) and compulsions (repetitive behaviors performed to reduce the anxiety caused by obsessions).
16. Carl Rogers’ client-centered therapy emphasizes all of the following EXCEPT:
A) Unconditional positive regard
B) Empathy
C) Interpretation of unconscious conflicts
D) Genuineness (congruence)
Answer: C) Interpretation of unconscious conflicts is a psychoanalytic technique, not a humanistic one. Rogers’ client-centered therapy is non-directive, emphasizing unconditional positive regard, empathy, and genuineness to create a safe therapeutic environment.
17. Systematic desensitization is a behavioral therapy technique based on principles of:
A) Operant conditioning
B) Observational learning
C) Classical conditioning (counterconditioning)
D) Cognitive restructuring
Answer: C) Systematic desensitization (Wolpe) uses counterconditioning — pairing a feared stimulus with a relaxation response — to replace the conditioned fear response. This is based on classical conditioning principles.
18. SSRIs (Selective Serotonin Reuptake Inhibitors) work by:
A) Increasing dopamine production in the brain
B) Blocking the reuptake of serotonin, increasing its availability in the synapse
C) Enhancing GABA activity to reduce anxiety
D) Blocking dopamine receptors to reduce psychotic symptoms
Answer: B) SSRIs block the reuptake (reabsorption) of serotonin by the presynaptic neuron, leaving more serotonin available in the synaptic gap. This increases serotonergic activity and is used to treat depression, anxiety, and OCD.
19. Electroconvulsive therapy (ECT) is MOST effective for treating:
A) Mild anxiety disorders
B) Severe, treatment-resistant depression
C) Personality disorders
D) ADHD in children
Answer: B) ECT is one of the most effective treatments for severe, treatment-resistant depression and acute suicidal ideation. It involves brief electrical stimulation of the brain under anesthesia and is typically used when other treatments have failed.
20. Albert Ellis’s Rational Emotive Behavior Therapy (REBT) is based on the idea that emotional disturbances result from:
A) Unconscious childhood conflicts
B) Irrational beliefs about activating events
C) Classical conditioning of fear responses
D) Chemical imbalances in neurotransmitters
Answer: B) Ellis’s REBT uses the ABC model: an Activating event triggers a Belief (often irrational), which leads to an emotional Consequence. Therapy focuses on disputing irrational beliefs and replacing them with rational ones.
21. The deinstitutionalization movement of the 1960s–70s resulted in:
A) A dramatic increase in the number of psychiatric hospitals
B) The shift of care from psychiatric hospitals to community-based treatment centers
C) The elimination of all mental health stigma in society
D) The development of the first antipsychotic medications
Answer: B) Deinstitutionalization shifted mental health care from large psychiatric hospitals to community mental health centers. While well-intentioned, it also contributed to homelessness among those who lacked adequate community support services.
22. A therapist who uses an eclectic approach would BEST be described as someone who:
A) Strictly follows psychoanalytic techniques
B) Only uses evidence-based cognitive-behavioral methods
C) Draws from multiple therapeutic orientations based on the client’s needs
D) Relies exclusively on biomedical interventions
Answer: C) An eclectic therapist integrates techniques from various therapeutic approaches (psychodynamic, cognitive, behavioral, humanistic, etc.) depending on what will be most effective for each individual client.
23. Which of the following personality disorders is characterized by a persistent pattern of disregard for and violation of the rights of others?
A) Borderline personality disorder
B) Narcissistic personality disorder
C) Antisocial personality disorder
D) Dependent personality disorder
Answer: C) Antisocial personality disorder (Cluster B) is characterized by disregard for others’ rights, lack of remorse, deceitfulness, impulsivity, and often a history of conduct disorder before age 15.
24. A person with PTSD would be MOST likely to experience:
A) Delusions of grandeur and disorganized speech
B) Flashbacks, nightmares, and hypervigilance following a traumatic event
C) Excessive worry about multiple everyday concerns
D) Cycles of binge eating and purging
Answer: B) PTSD is characterized by intrusive memories (flashbacks, nightmares), avoidance of trauma-related stimuli, negative changes in cognition and mood, and hyperarousal (hypervigilance, exaggerated startle response) following exposure to a traumatic event.
25. Which of the following correctly matches a treatment approach with its underlying principle?
A) Token economy — classical conditioning
B) Free association — cognitive restructuring
C) Systematic desensitization — operant conditioning
D) Exposure and response prevention — behavioral therapy for OCD
Answer: D) Exposure and response prevention (ERP) is the gold-standard behavioral therapy for OCD — the client is exposed to the anxiety-provoking stimulus while being prevented from performing the compulsive behavior. Token economy = operant conditioning; free association = psychoanalysis; systematic desensitization = classical counterconditioning.